Infectious Diseases Case of the Month
|
||||||
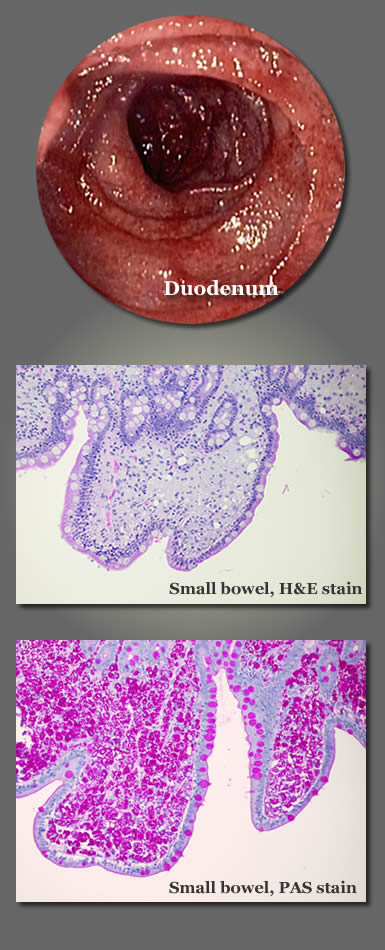 |
A 62 year old hispanic male was admitted to the hospital via the emergency room for severe diarrhea and weight loss. He had been having diarrhea, sometimes severe, for the preceding eight months with an accompanying forty pound weight loss. He had not had nausea, vomiting, abdominal pain, or fever, nor had he noticed blood in his stools. He did experience anorexia and an "aversion" to food. For perhaps the last five years he had been experiencing "rheumatic pain" (his term) which he characterized as muscle aches and swelling of his hands and fingers. He had been taking a steroid containing substance/medication he had obtained in Mexico for those symptoms. He was Mexican born but had been living in southern California for the preceding twenty years. He had been previously healthy and had been working as a "gardener" until his illness prevented him from doing so. Recently, family member living in Oregon had prevailed upon him to move to their home when his symptoms had become debilitating. At the time of his initial evaluation he appeared very ill, and his skin appeared hyperpigmented. He was alert and appeared to have normal cognitive abilities as best could be assessed via an interpreter. Cardiac exam was notable for a grade II/VI systolic murmur. He exhibited lower extremity edema. He did not have obvious synovitis. Stool was heme positive. Laboratory data included WBC 13.8 (H), Hgb 8.4 (L), albumin 2.1 (L), and normal hepatic enzymes. A CT scan of the abdomen and pelvis showed trace ascites but was otherwise unremarkable. Stools for enteric pathogens and ova and parasites were negative as were blood cultures. The patient was seen in consultation by a gastroenterologist who performed esophagogastroduodenoscopy and colonoscopy. Upon entering the small bowel and to the maximum extent into which he could advance the endoscope (into the jejunum), the endoscopist observed intense erythema and edema of the bowel mucosa with an indistinct villous pattern and "millions of dilated lacteals" (see representative photo of duodenum at upper left). The colon was normal, but examination of the terminal ileum showed findings similar to those of the proximal small bowel although the erythema was less intense. Biopsies were taken of the duodenum, jejunum, and ileum. All showed abnormal inflammatory changes as pictured at left (two lower images). Special stains for fungi and AFB were negative. A larger image of the periodic acid-Schiff (PAS) stained specimen can be seen by clicking here. An HIV antibody was negative.
Of the choices below what is the likely the cause of this illness?
|
|||||
|
Answer and commentary will follow submission of your answer. |
|||||