Infectious Diseases Case of the Month
|
||||||
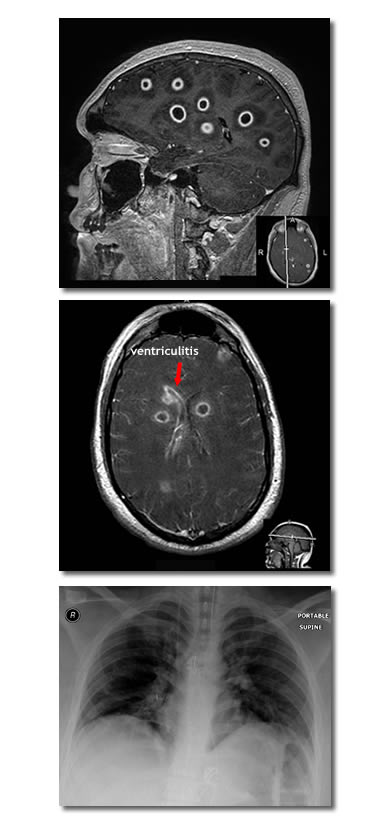 |
A nineteen year old white male was admitted to the hospital for meningitis. Previously healthy, he had not been feeling well for several days with complaints of headache, neck pain, and right shoulder pain. He developed confusion which prompted family members to bring him to the emergency room for medical attention. In the emergency room he was noted to have fever (100.2o) and to have a stiff neck. A lumbar puncture was performed (described as "traumatic" with only 2 cc of spinal fluid obtained) with the following results: WBC 4220 (67% PMN's, 27% monos), RBC 60, Glu 31 mg/dl, and protein 397 mg/dl. Gram stain of the CSF showed many PMN's but no organisms were seen. The patient was begun on IV vancomycin and ceftriaxone. He required endotracheal intubation because of progressive obtundation. A CT scan (not pictured) showed extensive but vague areas of hypoattenuation bilaterally in the cerebral hemispheres, the basal gangila, and the thalami. To further evaluate, an MRI scan was obtained which showed a dramatic picture of widely distributed ring enhancing lesions (two representative images are at left). The patient was estimated to have at least thirty to thirty-five of these fairly uniformly sized lesions and had evidence of right lateral ventriculitis. Also evident on neuro-imaging was sphenoid sinusitis without boney erosion (not pictured). Click here for larger views of the sagittal MRI image and the patient's CXR (bottom image at left). The patient was a native of Oregon and resided on the Oregon Coast. Approximately three months before the onset of his illness he had worked in a fish cannery where hake was processed. He had not directly handled the fish but had been involved in the final packaging process for shipment. Many co-workers were foreign born including many from Latin America. He was not an outdoorsman and specifically had not swam recently in freshwater. Family members were unaware of any HIV risks. The patient remained obtunded. Blood cultures and the initial CSF culture were negative. HIV antibody was negative. A transesophageal echocardiogram was negative for valvular vegetations or evident intra-cardiac shunt. He developed a rash and bronchospasm thought perhaps related to ceftriaxone. Meropenem was substituted. Multiple serologies and a repeat lumbar puncture were performed. Neurosurgeons were consulted but did not favor immediate brain biopsy for fear of low diagnostic yield and potential hazards to this young individual. Of the choices below what the likely the cause of this illness?
|
|||||
|
Answer and commentary will follow submission of your answer. |
|||||