|
A 53 year old white male was admitted to the hospital for shortness of breath and cough.
An otherwise healthy individual with neurofibromatosis he had experienced the insidious onset of shortness of breath beginning two to three months prior to his admission. Accompanying the shortness of breath was a non-productive cough. He had had no fevers, chills, or sweats. His breathing difficulties progressed to the point that he had difficulty sleeping. He eventually found it easier to sleep sitting up.
He sought medical care several times prior to his eventual hospitalization. He first presented to the emergency room approximately one month prior to admission and was found to be in supraventricular tachycardia. This rhythm spontaneously converted, and he was treated with diltiazem subsequently. He was also treated at that time with a five day course of azithromycin for his cough. Later when he developed peripheral edema and orthopnea, furosemide had been substituted for the diltiazem.
The patient had no previous history of cardiac disease including rheumatic heart disease or endocarditis. He had not had recent dental work and, in fact, had not been to the dentist for several years because of lack of means. He was a local scout-
master and had no history of intravenous drug use. He had not been suffering intestinal symptoms nor arthritic symptoms. He was not around animals significantly.
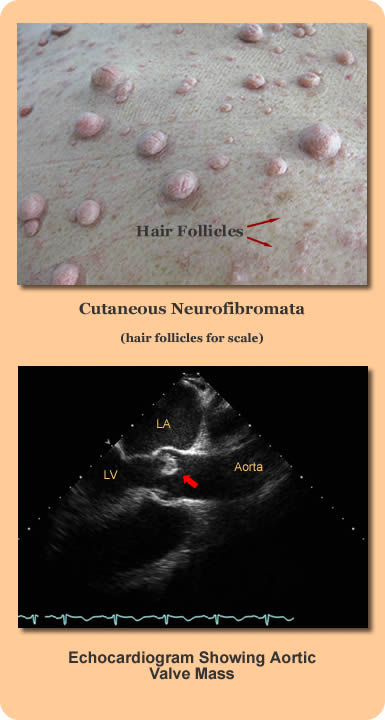
At the time of the patient's hospital admission he was afebrile but coughing, and had evidence of congestive heart failure clinically and radiographically. He had no apparent peripheral stigmata of endocarditis (splinter hemorrhages, Osler nodes, etc.) He had obvious extensive cutaneous neurofibromata (see image upper left). Laboratory data included WBC 15 (H), Hgb 12.9 (L), Plts 300, ESR 40 (H); LFT's were normal. A trans-esophageal echocardiogram showed severe aortic regurgitation and a 1.8 x .8 cm hypermobile mass along the leaflets of the noncoronary cusps of the aortic valve (see image lower left).
A cardiac surgeon recommended aortic valve replacement because of the degree of valvular incompetence. Four blood cultures were obtained and the patient was begun on IV ceftriaxone for possible subacute bacterial endocarditis.
|