Infectious Diseases Case of the Month #3 |
|||
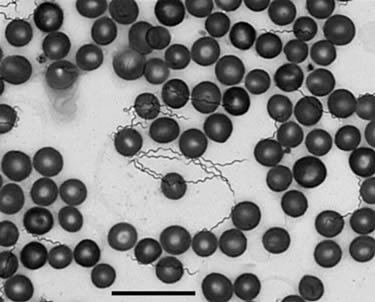 |
A 62 y.o. white female was seen in clinic for a several week history of episodic fevers, malaise, myalgias, and prostration. Episodes lasted several days with intervening periods of relative well being lasting approximately one week. She had had three such cycles of illness at the time of her evaluation. The patient had previously been in good health. Ten days prior to her first episode of illness she had spent several days at her family cabin on Lake Roosevelt. Lake Roosevelt, in north central Washington, is a reservoir formed by the damming of the Columbia River by Grand Coulee Dam. The patient had swam in the reservoir and gone for lengthy hikes about the property. She could recall no specific insect exposure. Laboratory evaluation was notable for leukopenia (WBC 2.7) and thrombocytopenia (plts 76). Liver function tests were normal. She was feeling well when seen in the office. Had she been seen during one of her episodic periods of illness, her peripheral blood smear might have appeared as the one at left. Photo courtesy of Tom Schwan, PhD, Rocky Mountain Labs, NIH/NIAID |
||
What bacterium is the most likely cause of her illness? |
|||
 |
This patient likely had relapsing fever, a tickborne illness endemic in regions of the western United States. Tickborne relapsing fever (TBRF) is caused by any of several species of the genus Borrelia; in the United States the majority of cases occur in western states and are caused by B. hermsii or B. turicatae. The bacteria are transmitted to humans by the bites of argasid (soft) ticks of the genus Ornithodoros. Unlike in the case of hard shelled ticks such as Ixodes (that transmit the agent of Lyme disease), Ornithodoros ticks feed for less than one hour, typically at night, and the bites are painless and usually unnoticed. Although the primary tick hosts are chipmunks and other small rodents, humans may be bitten when they frequent caves or rural cabins accessible to rodents. TBRF is clinically characterized by recurring fevers whose median duration is 3 days with alternating afebrile periods with median duration of 7 days. Fevers may be accompanied by headache, rigors, diaphoresis, arthralgia, myalgia, dizziness, nausea and vomiting. Without treatment up to ten relapses may occur. Diagnosis is made by demonstration of spirochetes on peripheral blood smear. Paired acute and convalescent antibody titers can be used to confirm the diagnosis when culture or blood smear is not available or is non-diagnostic. Tetracyclines or penicillin are the drugs of choice for treatment. Jarisch-Herxheimer reaction is said to be common after the initiation of therapy. The case cited here is one of probable TBRF as the diagnosis was made on the basis of clinical symptoms, epidemiology, and serology. An IFA titer was greater than or equal to 1:256, and Western blot was positive for GlpQ antigen, a protein specific for relapsing fever spirochetes. The patient responded well to doxycycline without apparent Jarisch-Herxheimer reaction and suffered no further relapses.
|
||
| Home Case of the Month ID Case Archive | Your Comments/Feedback | ||