Infectious Diseases Case of the Month #12 |
|||
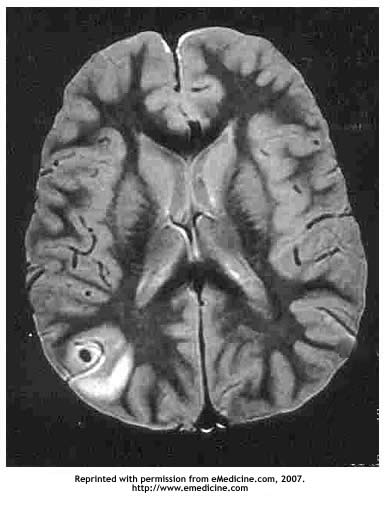 |
A 25 y.o. hispanic male was admitted to the hospital for a seizure. Previously in good health he had been born in Mexico and lived there until eight months prior to admission when he and his wife emigrated to Lake Chelan, WA (map) where he was employed as a laborer in the fruit orchards. He was married and his wife had immigrated with him. A couple of weeks prior to admission he had fallen from a ladder while picking fruit sustaining an injury to his knee necessitating orthopedic evaluation and knee immobilization.On the date of hospital admission he had developed a left frontal headache and subsequently experienced the onset of involuntary shaking of his left upper and lower extremities. He did not experience loss of consciousness. A CT scan showed a focal area of low density in the right parietal region. A subsequent MRI scan showed a 1-2 cm cystic structure with central opacity with surrounding edema similar to the MRI scan featured at left. The patient was afebrile with otherwise normal vital signs. Examination was unremarkable. He denied sexual promiscuity, IVDU, or other HIV risk factors and had not had recent prolonged respiratory symptoms. He was begun on dilantin and dexamethasone, and neurosurgery consultation was obtained. He underwent neurosurgical resection of the cystic abnormality. Prior to surgery these labs were obtained: WBC 13.7 (with normal differential), Hgb 13.3(L), Na 139, Ca 10.4. An infectious diseases consultation was requested after initial review of the pathological specimen. |
||
What micro-organism most likely was the cause of this patient's cystic brain lesion? |
|||
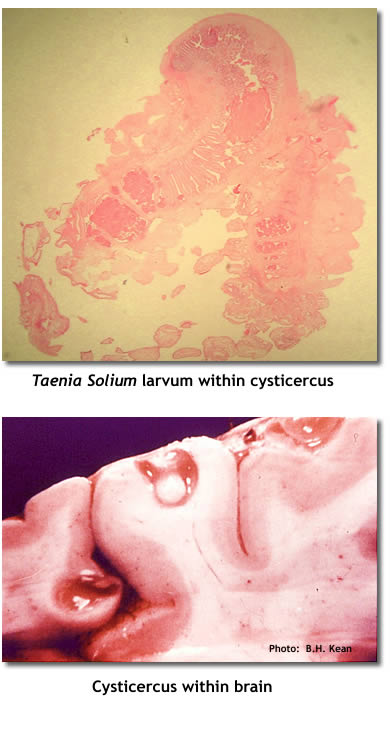 |
This patient had neurocysticercosis secondary to Taenia solium. Pictured at top left is a section through the Taenia solium larvum within the grape-sized cysticercus resected from the brain of the patient described in the previous vignette. Taenia solium, the pork tapeworm, has a complex life cycle. Humans infected with the adult tapeworm shed eggs in stool which are subsequently ingested by pigs, the usual intermediate host for Taenia solium. Embryos emerge from the eggs and disseminate to various tissues where the encysted larval stage (cysticercosis) develops. When humans ingest raw or undercooked pork containing cysticerci, the cycle is completed when the larval forms attach to small bowel and mature into adult tapeworms. Unlike other cestodes infective to man, humans can also be intermediate hosts for Taenia solium. Through ingestion of Taenia solium eggs (or via auto-infection of persons parasitised with adult tapeworms) cysticerci can develop in various human tissues just as in pigs. When cysticerci parasitize the central nervous system, the disease is known as neurocysticercosis. An autopsy image at lower left (not from the current case) shows the gross appearance of a CNS cysticercus. Neurocysticercosis is the most common cause of new onset seizures in certain parts of Mexico and Latin America where the disease is endemic. Surgery as was described here is not a typical means of diagnosis or treatment of this disease. Rather, diagnosis is made clinically based on epidemiology, appearance on neuroimaging, and serology. Anticonvulsant therapy is the primary treatment of persons identified with cysticercosis as a consequence of new onset seizures. Specific anti-parasitic therapy may also be employed, but there remains controversy as to its benefit. Neurocysticercosis can be a very serious, sometimes fatal, disease particularly when cysticerci are located such that they cause obstructive hydrocephalus or are so numerous as to cause diffuse encephalitis. The other micro-organisms listed in the prior vignette (see original format) can also cause central nervous system disease. Toxoplasma gondii can cause ring enhancing (non cystic), usually multiple, lesions typically in persons severely compromised with AIDS. Paragonimus mexicana, the lung fluke, most commonly parasitizes the lung, but can cause cystic lesions of the brain that could be difficult to distinguish from those caused by Taenia solium. Gnathostoma spinigerum, a nematode known to cause disease in Mexico, can cause a syndrome of eosinophilic myeloencephalitis due to a migration of larvae into the central nervous system. Mycobacterium tuberculosis can cause meningitis and more rarely, mass-like tuberculomas. Tuberculomas would not tend to be cystic in nature. Ref: Sorvillo, F.J., et al, Deaths from cysticercosis in the United States, Emerg Inf Dis 13(2):Feb 2007, pgs 230-235. |
||
| Home Case of the Month ID Case Archive | Your Comments/Feedback | ||